‘Apparent Disdain’ For Patients Linked To Minneapolis VA Suicide
Here is what you need to know about the newest IG Report after one veteran committed suicide at Minneapolis VA after making obvious suicidal comments to VA staff.
The Minneapolis VA mental health team is run by a doctor with an “apparent disdain” for patients seeking mental health care at the facility. In 2018, there were two suicides in the press, both of which could have been avoided if staff paid attention to basic English.
I live near the Minneapolis VA and have sought care from them a few times.
Some of the folks at the Minneapolis VA are great. Some are not. Dr. Michael Dieperink should be completely embarrassed after the IG Report calling out his inability to properly train staff to prevent suicide.
Sporting a 1-star rating, reviews on Healthgrades.com called Dr. Dieperink “a total quack” and “Dr. Michael Dieperink is a horrible person: arrogant and condescending. He has little interest in the wellbeing of his patients and offers nothing to the field of psychiatry.”
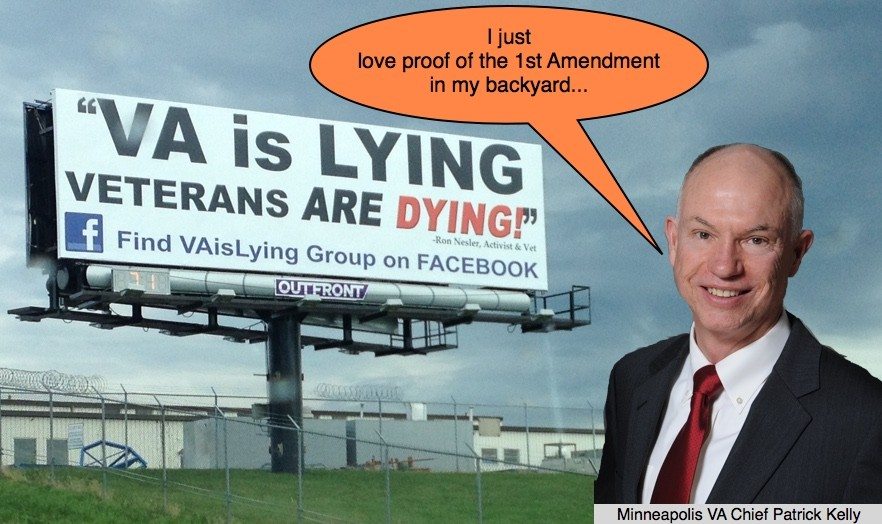
Head of the facility, Dr. Dieperink’s boss, Patrick Kelly wrote, “Suicide prevention is the VA’s number one clinical priority, and this tragic event has greatly impacted the family and the staff at the Minneapolis VA Health Care System.”
Really?
Veteran came into the ER suffering from withdrawal symptoms from opioids and benzodiazepines. How many veterans meet this description?
VA gets you addicted to a substance. They then cut you off.
The veteran tells staff he has thoughts of suicide and homicide. While an inpatient, he told a dietitian, chaplain, and medical resident, “I came here to die,” “I want to die” and, “I wish that someone could give me a dose of morphine so I could die.”
Nurses, doctors, and anyone with ears knew the guy was suicidal.
Two hours later, the veteran completed his suicide after disappearing from the hospital.
So, why was he not in 72-hour hold?
Distain For Veterans?
My friend and attorney Brian Lewis has some ideas that I wanted to share with readers curious about what’s going on within the Minneapolis VA mental health department in reference to the Stars and Stripes article about the IG Report.
Full disclaimer behind the sign above. Brian and I were part of the push to publish that billboard at three locations surrounding Minneapolis VA back in 2015. It cost $15k for three billboards for one month. Worth every penny.
RELATED: Leaked VA Email Complains Of Veteran 1st Amendment Activity
Many VA employees complained to Patrick Kelly about the sign and even asked him to make us stop. He literally had to write an internal memo to those employees complaining to remind them that veterans enjoy the 1st Amendment just like every other American who did not fight to protect it.
RELATED: VA Is Lying Billboard Goes Up Across From Pheonix VA
Here is what Brian Lewis had to say about the “apparent disdain” of the head of mental health that led to the malaise leading up to the suicide:
OK, so here’s a point of view from someone who uses the failure called the Minneapolis VA Health Care System. It wouldn’t have mattered one bit had God and everyone took the proper actions. The Mental Health Services Department at this supposed medical facility falls beneath even the Veterans Health Administration (VHA) – U.S. Department of Veterans Affairs’s usual standards of malpractice care. When the rest of the hospital sees that the Mental Health Services Department is in disarray, disengaged, and disinterested in their patients, why even bother to send a consult over?
I believe Dr. Michael Dieperink, the Mental Health Services Department Head, has virtually zero interest in patients. His apparent disdain for patients radiates down through the chain of command and has infected professionals throughout the department. The staff appears to be overall more concerned with numbers and metrics than actually providing patient care that aligns with patient goals. Even inside the #PTSD Clinical Team, the staff appears to be more concerned with evidence-based practice, avoidance of alternative therapies, and ensuring patient desires for their care are ignored. Thus, I find it hard to believe the veteran in question actually received mental health care that was appropriate to needs.
When the new Director of VISN 23, Mr. Robert McDivitt, first came aboard, I asked him at the VA Town Hall if he had any plans of conducting independent oversight of the Minneapolis VA. He hemmed and hawed around the question for a good minute, but the answer was no. CAPT Pat Kelly has proven over the course of several years and at least two separate deaths that he is unfit to lead a patrol to the latrine, much less a major medical center to a course correction it badly needs. Isn’t it time to dump a zero, U.S. Department of Veterans Affairs? The #veterans you serve deserve better.
RELATED: VA Is Lying Signs Show Up In Chicago
Shocking IG Report Summary
Hold what Brian had to say in your back pocket for a second and compare that to what the agency summarized in the IG report:
The VA Office of Inspector General (OIG) conducted a healthcare inspection to access care coordination for a patient who died by suicide while admitted to an inpatient medicine unit at the facility. The patient was assessed as heightened but not imminent risk for suicide.
Facility Emergency Department staff failed to report the patient’s suicidal ideation to the facility’s Suicide Prevention Coordinator. Two consulting staff members and an inpatient registered nurse completed required suicide prevention training but failed to involve clinicians when the patient verbalized suicidal thoughts and warning signs. Two of the three staff documented the patient’s suicidal thoughts and warning signs in consult results notes, but the OIG did not find documentation that the inpatient medicine resident reviewed or acted on the consult results.
During an internal review, the facility’s root cause analysis team did not interview staff members involved in the patient’s care. The internal review team identified many lessons learned for which the Veterans Health Administration (VHA) does not require action items. VHA does not provide written guidance on the identification of lessons learned, related action expectations, and how to distinguish lessons learned from root causes. The absence of formal guidance may have contributed to the team’s failure to identify critical actions in the prevention of adverse patient events.
Facility leaders did not make an institutional disclosure to the patient’s next of kin. The Patient Safety Committee and the Quality Management Council meeting minutes did not document deliberations and track actions to resolution.
The OIG made a recommendation to the Under Secretary for Health related to written guidance for lessons learned, and six recommendations to the Facility Director related to Suicide Prevention Coordinator notification, a review of the patient’s care, consult results, institutional disclosure, the root cause analysis process, and documentation of meeting minutes.
RELATED: AFGE Spying On VA Is Lying Group
Is Patrick Kelly Being Honest?
Digging a little deeper, the lack of consideration and failure to adhere to standard suicide protocol make me think Patrick Kelly is either totally ignorant about his staffs’ disposition toward suicidal veterans or lying.
RELATED: VA Secretary Meets With VA Is Lying Group
Here is what IG said from the brief patient summary buried within the report:
The patient was in their sixties at the time of death by suicide in spring 2018. The patient used a central nervous stimulant for more than 30 years. Starting in 2006, the patient received mental health treatment at another VA medical center’s community based outpatient clinic (CBOC). The patient established sobriety and mood stability for over 10 years through treatment including a combination of an antidepressant and an antipsychotic medication. In 2017, the patient transferred care to one of the facility’s CBOCs. The primary care provider diagnosed the patient with major depression and history of substance use in remission. For additional patient case summary details related to pre-spring 2018, see appendix A.
On a day in spring 2018 (day 1), the patient’s public health nurse informed the facility CBOC team that the patient had been taking leftover medication (benzodiazepine 1) and had run out. The nurse described the patient as “a little unsteady” and reported that the patient had “a rough weekend.” The CBOC nurse called the patient who denied suicidal ideations although reported feeling more depressed. The patient agreed to come in the following day. On day 2, the patient presented to the CBOC. The primary care physician documented that the patient abruptly discontinued benzodiazepine 1 one week prior and had been trying to decrease use of opioid medication 1. The patient described dizziness, nausea, vomiting, and visual hallucinations but denied seizure activity. The patient verbalized a desire to stop taking all narcotic medications. The physician urged the patient to go directly to the facility’s Emergency Department, but the patient declined and chose to go to a non-VA Emergency Department instead. The non-VA Emergency Department provided intravenous fluids and discharged the patient home. On day 3, following a fall, an ambulance transported the patient to a non-VA Emergency Department where the patient was treated with opioid medication and intravenous fluids, and discharged to home. The patient called the CBOC on day 4 requesting help with opiate and benzodiazepine withdrawal symptoms. The patient agreed to go to the facility Emergency Department and the CBOC nurse called ahead to provide communication regarding the transfer of care.
When the patient arrived in the Emergency Department on day 4, the triage nurse described the patient as disoriented and reported that the patient denied thoughts of self-harm or harming others. However, the patient told the Emergency Department staff nurse about thoughts of suicide and homicide, and acknowledged having a gun at home. The patient told the Emergency Department evaluating psychiatrist that the patient would “definitely end it,” if “discharged home tonight and go into opiate WD [withdrawal].” The patient reported having a loaded gun and “a suitcase” filled with “old medications” at home. The evaluating psychiatrist recommended inpatient admission for observation and treatment of depressive symptoms, suicidal ideation, living alone with ample access to means of suicide, mild cognitive impairment, and withdrawal symptoms. Due to a lack of available facility or community psychiatric beds, the psychiatrist recommended admission to a medical unit and stated, “[n]o need for 1:1 sitter,” because the patient professed being able to remain safe on a medical unit and agreed to alert staff to any thoughts of suicide or self-harm.
On day 5, the patient was admitted to an inpatient medical unit. The inpatient medicine resident noted that the patient was intermittently agitated and stated, “I want to die.” The resident prescribed a medication for agitation and anxiety. Later that morning, the patient told the dietician, “I wish that someone could give me a dose of morphine so I could die.” The patient also told the chaplain about the wish for morphine to die, as well as feelings of guilt and being “unforgiveable.” The following morning, the resident documented that the patient “feels much better” but continued to express suicidal thoughts. Later that day, a nurse documented that the patient endorsed feeling depressed but denied suicidal ideation.
On day 7, the psychiatrist noted the patient’s depression and confusion, but the patient denied suicidal ideation and verbalized not wanting to die. The patient was found to have “significant” cognitive impairment, and the patient expressed a desire to go to a nursing home at discharge. The psychiatrist assessed the patient as being at heightened, but not imminent, risk for suicide, and did “not see need” for the patient’s transfer to an inpatient psychiatric unit but would reassess once discharge options were determined. The psychiatrist deferred completion of a safety plan until the patient was ready for discharge. That evening, the chaplain documented that the patient thought “[the patient] may die soon.”
On day 8, the occupational therapist assessed the patient as having mild to moderate cognitive decline and recommended an assisted living facility placement at discharge. Mid-morning, an inpatient nurse overheard the patient on the phone telling someone that the patient was going to die in the hospital and “I want you to have the seven acres for all the help you have given me.” The patient was not in the hospital room approximately two hours later. and the nurse did not find the patient during a search of the unit. The nurse had the patient paged overhead, but the patient did not return. Forty-five minutes later, the nurse contacted the Assistant Nurse Manager, who then informed the VA police that the patient was missing. Approximately 30 minutes later, the VA police received a call that a patient attempted suicide. Emergency responders provided cardiopulmonary resuscitation before the patient was taken to a non-VA Emergency Department, where the patient was pronounced dead.
RELATED: VA Policy, DHS Monitoring VA Is Lying Group
Brain Tumor And More
If you are still reading, you are my kind of advocate. Here is the final bit that jumped out at me that most folks will not appreciate. The veteran recently had a meningioma tumor:
The patient was in their sixties at the time of death by suicide. After military discharge, the patient used a central nervous system stimulant for more than 30 years and established abstinence in 2006. The patient reported mood stability on a combination of an antidepressant and an antipsychotic medication for more than 10 years. In 2006, the patient established care with the VA after receiving non-VA mental health and substance use disorder treatment and was diagnosed with major depressive disorder, recurrent, severe, and substance use remission. The patient completed a one-month VA domiciliary admission in 2007 and continued mental health treatment at a VA medical center CBOC.
In summer 2017, the patient transferred care to one of the facility’s CBOCs. The primary care provider diagnosed the patient with major depression, and history of substance abuse, in remission. The psychiatrist continued the patient’s six active medications for treatment of anxiety, insomnia, chronic pain, depression, and stabilization of mood. Prior to this episode of care, the patient was prescribed medication for anxiety and insomnia, but that prescription was discontinued because the patient was also taking medication for sleep.
In fall 2017, the patient presented to a non-VA hospital Emergency Department with a complaint of new onset headaches for three days. Brain imaging revealed a 4-centimeter brain mass consistent with a neoplasm and the patient was directly admitted to the facility. During the admission medication reconciliation, the patient reported having “extra bottles” of benzodiazepine 1 and taking the medication at bedtime for anxiety and sleep despite having been told not to by a provider. The patient was discharged three days later, with a plan to return for tumor removal surgery approximately a month later.
Prior to the scheduled surgery, the patient’s public health nurse contacted the CBOC primary care nurse with concerns about the patient’s nonadherence with the prescribed medication regimen.40 The public health nurse reported that the patient was not taking medication as prescribed and that the patient “is very calm in the mornings, but by evening, [the patient] is agitated; tells nurse and family that [the patient] sees bugs in [the] house again.” The primary care nurse recommended that the public health nurse contact the neurosurgery team.
Ten days later, the patient was admitted for a craniotomy and meningioma resection. The pathology report confirmed a meningioma diagnosis. During recovery, the patient exhibited impairments in balance, mobility, and completion of activities of daily living. The patient was admitted to acute inpatient rehabilitation four days after surgery. Approximately two weeks later, the interdisciplinary treatment team met with the patient’s family members. The interdisciplinary treatment team described improvement in the patient’s activities of daily living and ability to walk, and recommended 24-hour supervision, cessation of driving, and a family member to stay with the patient for a week to help with home equipment set-up and development of routines after discharge. The physician recommended that pain medications continue to be tapered on an outpatient basis. The patient repeatedly refused to stay with family members or to discharge to a supervised facility. The patient was discharged to home six days later, with instructions to follow up with primary care, the traumatic brain injury clinic, radiation oncology, neurosurgery, mental health, and with the home public health nurse.
The patient met with a psychiatrist for an intake evaluation a month later. During that visit, the patient described a “pretty good” mood and denied current suicidal ideation, though the patient continued to report insomnia and memory problems. The psychiatrist diagnosed the patient with mild neurocognitive disorder; major depression; recurrent, moderate, delusional disorder; and substance use disorder in sustained remission. The patient reluctantly agreed to discontinue benzodiazepine 2, increase the sleep medication, and continue the other medications, including sustained-release antidepressant 1 daily. At the patient’s follow-up visit the patient admitted to continuing benzodiazepine 2 despite instructions to stop taking it, due to fears of worsening insomnia. The psychiatrist repeated the rationale for discontinuation and told the patient the benzodiazepine 2 would not be refilled. The patient again described a good mood and denied suicidal ideation. The psychiatrist planned to increase the sleep medication dosage, discontinue benzodiazepine 2, and continue other medications at prior doses. The last prescription for antidepressant 1 was a three-month supply ordered in late 2017, but it was discontinued by pharmacy 21 days later. Approximately a month later, neither the mental health nurse’s progress note nor the medication reconciliation note included antidepressant 1. The patient did not attend the scheduled psychiatric follow-up in spring 2018.



I’m fighting vehemently to identify and dismantle the metaphorical illusion that expresses to Veterans, their families, the public, and our government, that things are peachy at VA facilities across the United States and abroad. There is no excuse for the lack of action taken to create a stable environment that offers nothing but the best for our Veterans. The “VA Mafias” days are numbered if I have any say in it. It’s shameful to operate under a system that allows anyone to do a disservice to over Veterans and their families. The most noble cause in government will not go unnoticed as long as we all stand for what is right concerning the promises that we made when they answered the call to secure the freedoms that we all experience in this great nation.
The hearing are worthless and you can have all the meeting you want. Congress can’t even keep there office at VA! All systems are broken. The doj was selling whistle blower complaints! US attorney was hiding and destroying evidence on death penalty cases. ALL government branches are corrupt and don’t care about the people! Even Social Security was found guilty for firing a veteran for being disabled. No accountability as our peoples lives are destroyed!
Here’s a brand new article out by vets for vets:
*”https://www.foxnews.com/us/va-grading-system-veterans”*
What do y’all think about “removing the star system”?
You can tell who the VA staff and cheerleaders are leaving comments.
Locally they all stopped grading sites, abilities, or leaving comments for civilian care here or any clinic or MD. Not the reports or comments they want to hear or allow other potential test rats, consumers, to read about.
Seems it’s just another failed grading system by the VA. Stars don’t cut it and “detailed” systems won’t either. Veterans or those wronged are not, will not, be in control of editing, censoring, etc. It will go the way of local attempts to grade health care, staff, MDs, etc., edited, blocked, deleted, shadow banning fake outs, then trashed finally. As usual ‘no negatives allowed,” no truth. There are more important issues to be discussed and acted on besides ‘grading systems.’ Same crap different day, different years, SNAFU. When they get complaints just act on them instead of playing pass the buck games, messing with records, refusing to give a team-mate a black eye stamp on their work records… the go on the attack with the games.
That video refuses to play for me too.
No reply Ben. Yes agree with RF blocker. On my own. Going around. There is the saying thinking out of the box. How about thinking without an existing box in place? Plow through the mainstream. Eliminate all labels. Pragmatic. Practical. Deliver results. Ben, President Trump is 100% correct. Too much process. The federal government is too big for process. The VA wallows in process. This is why results and resolve are never delivered. Process is all about research, evaluate, and subjectivity. Any issue can be evaluated to both positive and negative infinity which means never ending. This is why zero accountability exists in the VA. They spin it all around the globe. Ben, going back to the Voc Rehab survey. Why do they bother? So they can say they are doing something which is really nothing. Because they will not acknowledge the results. Why the survey? Why do they call on a Saturday? Oh yes, one cannot return the phone call. All the lifetime top civil service govt types need to somehow be removed. They are the problem. Because a President can only be elected for 2 terms. The Supreme Court could make a dent in improvement if more Constitutionalists are put on the court. Republican controlled House of the correct type Republicans are elected. And yes there are correct type Republicans. The ones who are not panders, who are not liars, and who are not theives. I am referring to the ones who try to follow their conscience and the law. Examples, Republican Tom Cotton, Republican Devin Nunes. Law abiding. Principled. Honorable character. Benjamin, the blame belongs to the politicians. My part in it was I became sick due to Navy guinea piggliness. ? I do not care what they do? I have had enough of most of them. I want them to eat that process. Process keeps all situations and people stuck. Best.
I’ve been on a little sabbatical from FB and online social stuff. Plus so many books to read, the real Constitution, it’s meanings/intent too, and little time left. Being censored, banned, and attacked by all means by the many deceivers doesn’t help either especially when we live in a new land near full of the corrupt or corruptible, deceivers and flat out communist, countless activist, or foreigners. Plus after many many years of trying to deal with corruption or exposing evils seeing how deep the corrupted roots go, and no-one in power positions, their aids or secretaries, et al, not giving a crap about us doesn’t help matters either. We tend to just make more enemies for whatever reasoning they have.
Let’s quit playing games and get really real.
For one those behind so-called social groups to help vets like FB pages, this group or that group, this bike club or that one, ALL the VSOs, or “VA is lying,” is BS and no help at all. More for information gathering and to help gas-light other vets rather than helping. They all have their own little side agendas or groupies and don’t care about much else but maybe stuffing their own egos or pretending to be doing something for all. They all too will protect their own, the nepotism, family members, cliques, clans, tribes, connected associations/unions in health care or out, their secret societies/clubs, etc. Yeah, I got proof of that too… in my state and community. Indiana is near full to the brim of two-faced lying asshats but love donations and playing the game. Oh, while they get or claim to be getting their pain meds and acceptable health care from the VA or in their locations of course. Hope I ruffled some corrupt feathers out there too. That includes larger so-called veteran help law firms nation wide that claim to help vets with ANY issues. Liars, no better than the ACLU or their lying counterparts of media or politicians of any flavor.
I also have to laugh at those thinking your small firm, Ben, can take care of or handle all our issues out here and licensed to do so nation-wide.
I also know what “Veteran Patriot” is talking about and why I now use a Body Cam. Now use a RF blocker for the cell phone. Pretty sad when we get into positions where strangers can know where we are unless followed, them coming up seemingly making remarks to let us know they know everything there is to know about us including health care to banking accounts or money on hand. Or questioning us/me about disability plates or parking in blue areas and why. American privacy and having rights and freedoms? Horse shit. And people still want to play the back and forth two political party blame games, funny.
Oh, got more bone chips working out of the gums too years later from the VA shattering my jaw pulling a tooth. While civilian dentist and oral surgeon refused to X-ray my jaw not wanting to get involved with VA crap or malpractice. “Professional courtesies.” Like with the VA more file info manipulations and info omissions too. Real nice those country clubbers, medical board asshats and “professional” are…in Indiana and nation-wide. Cough burp fart.
Solutions? None. Not for all and especially in some locations and states, for sure.
Most people can’t wrap their tiny brains about the levels of corruption we deal with or have. That includes major radio hosts I’ve called or contacted. They have faith in ‘professionals”, the VA or gubbermint or their locals. They can’t begin to perceive the networks of corruption and covering-ups or how scum want to stay employed even though they know who or what they are working with or around. The know-it-alls just have their own life experiences to draw on, whats on TV, and living the fast lane to stop and consider just what the hell is being told them. Goes in one ear out the other then DUH. Oh don’t offend or harm their buddies or special interest group or masters. Well write the VA or a politician, state agency, or media head. Insert big laugh here.
Hi T – been a while. I do the best I can with the meager resources at my disposal, but it takes money to assemble a well-funded legal team and travel to DC on a regular basis. The culture of “free help” is part of the problem. Many veterans still demand all help should be free, as do VA and VSOs, so you get what you pay for – – free help ≠ best help.
Howdy Ben, hope all is well and healthy on your end.
Totally understood. I can also fully understand what you may go through in your processes of doing what you do including loss of family time, all the hassles, along with the rest. Plus those not liking what you do one little bit. I do what few others do and attempt to put myself in their position, family to geological areas, other data like trying to network with others of like minds or kindred spirits, motives.
Personally I don’t and never expect anything for free. Learned my lessons well over the many years just from some ‘free consults’ from various professionals. Chuckle. Turned out not to be so free even for ten minutes to get one question answered. Our issues today are far different from me in my younger days of like putting roofs on houses or working ‘free’ for selected folks who needed help, that do-gooder stuff. Plus countless hours of other volunteer free work from the gutters up. Not much real gratitude for ‘free’ doing for others either. Majority just want/expect more and more of it for life.
Or what attorneys claim locally about them doing a claimed required percentage of pro bono works. Typically here it’s for less involved family issues, small claims, or female stuff. The cheaper, more local, and easy thing to do. Not so easy or cheap to do with what we, or you face. Expecting people… should just check out travel, meals, lodging costs alone, then try to complain. In addition to other issues.
I can’t even hire videographers willing to do their thing for me out in the streets with my bull-horn and signs doing my little thing. They’ll all do weddings, funerals, activism of all sorts… but not me. Including college students I’ve talked to fearing involvement. All seem too afraid and not wanting involvement. Same with local attorneys (All called) that refuse to write one simple letter to see why Union Health Care here, professionals refusing X-rays to getting needed copies of those medical files they can seemingly refuse patients of, or X – VA patients from getting. Same with journalist I’ve offered to pay for some investigations while out in the streets, to the private eyes that run off too and join the evil ones. Plus give them more info on me or what I am up to.
I have to go out of county to get my household needs done I can’t do any longer. Funny stuff really. Even to clean a septic system and that’s getting bad and shows some real community hatred and shunning. With all the clowns thinking it really upsets me or supposed to drive me over the edge. I got some news for em. lol
Do what KrisAnne Hall and husband does while teaching the real Constitution. They’ve traveled to DC, get donations, plus whatever. But they’ve been doing this a while and not just starting out. They too are not well liked or supported as they should be. “https://krisannehall.com/”
Hell, I donate to her and will to you too even if I don’t live long enough to reap any benefits. Anyone willing to go to DC in that stench to do good earns my donations and purchases. Just a pity I’m not a millionaire or billionaire. Not afraid of doing without, not playing good little consumer, not keeping up with the Jones’s or putting some bills on hold either.
I’ve offered countless people online and off to get a free speech veteran forum up minus attack dogs, control freaks, trolls, agents, and no-one with the ability or time care to do it. Too many want everyone else to do it and all for free, but would surely use it once in place.
Yeah, I know all too well about the VSOs and other not wanting to risk their free stuff called tax dollars or donations for free stuff through city, county or state governments. They won’t help many out here or have, but will surely get those tax dollars to put a little American flag on my grave once a year.
Take care Ben, and of yours. I think some serious storms are brewing and coming our way in the USA. While illegals to refugees get their free stuff we paid for and can’t attain. Yep, everyone wants free stuff and want it now, or expect us to give everything we have to any others claiming they deserve it more, more needy, than us. Odd how so many huge law firms, countless others, help those kind too but refuse do anything for vets or Americans.
Dr Hartnett,
I suggest writing a Preamble to the Document you mentioned- something like a Bill of Rights to follow and of course if we are going to send it to King James and His Crony Court we will need a Constitution. The gestalt of all of this becomes the forming of a new government and that suggestion by itself will get us on every watch list as dangerous people.
The problems we Vets know about are exemplars of Crony-Capitalism gone off the rails. Stuff like “Thrush” from using inhalers and poor patient education are so common in the VA its as if they want us to hurt ourselves. I myself had the same issue in Chicago- the Pulmonologist who prescribed an inhaled steroid said “you have to rinse your mouth after using this” He never said brush your teeth, gargle and rinse 3 times. I had to tell him that is what the patient needs to do and he was surprised. Others like MD Betsy Ross are quick on the trigger to fry your brain with ECT in Albuquerque ( say no to that stuff, brothers ). Then there are the Prozac like drugs which chemically castrate a person in every way. Those dry orgasms do more than hurt the patient.
Such dismantling of our armed forces after service is beyond Brave New World. Wouldn’t Jackass Juilian Huxley and his scumbag brother be proud of the VA. In the upcoming future I’m sure they will attempt permanent placement of electrode wires in the brains of Veterans. I mean at this point why not turn us all into ass-licking Androids?
I hope somebody up top reads this stuff just so they know that in the end some of will still be rational enough to put out the trash. Do not let them take our 1st and 2nd amendment right s from us . Oh yeah and by the way , there are rumors that the VA has secret hit squads operating off the Reservation inside the US using drugs and electronics (Radio Frequency: 388Mh, Sub-sonics: 10- 18 cps & Ultrasonics: 18KHz-67KHz) to wipe out the Veteran population.
I surely don’t mean to make anyone more worried but watch out because this is now way beyond 1984 Big Brother, the current state is the equivalent to BF Skinner’s Skinner Box with everyone on the internet participating in operant conditioning mode. This was the CIA’s grand design: one big Skinner Box with everyone in their little chambers chatting like Rats on the internet while the NSA and their Huxley wannabees fucking us over. You can expect AI modules designed for Doctors not patients and those same modules will do one thing first- protect the Doctor from a malpractice suit. Medical Logic modules will be developed to assist clinical decision making with this in mind first: do no harm to the filthy VA pigs that put their hands on you the patient. If you think you are being followed around town , get yourself a RF Blocker pouch for your phone- it will stop the Cell Tower pinging your location.
As you can see this is not going down well with me because I have worked in the field and i know where this is headed, and its not good.
Thank you for posting this.
#Veteran Patriot,
Have you seen where the “82nd Airborne” is NOT being allowed to take their cellphones overseas to the Middle East.
There’s no law against it. It’s being implemented by higher ups! They claim it’s for “security purposes”, where the enemy could possibly locate anyone!
I believe it’s so these young servicemen and women won’t be learning the truth about how screwed up our Republic has become!
What are your thoughts!
Elf Brother,
Thanks for the info on the 82nd, our Warriors. This is typical of the antiquated military. Keeping Our next Veteran generation in the dumb down mode. The DOD learned a long time ago how to control people by asserting complete control over the ” Semantic Interface”
Take a look at Websters definition: it means everything that is graphical, written, spoken, signed or otherwise communicated. The Military will corrupt even the most basic reality by altering the messaging between individuals . Once you have complete control over the semantic interface you can get people to do anything. This is also how the VA works- the same processes of control by the same people circling the drain at the bottom of the revolving door. For example: if you look this control graphic: a triangle with Communication as the base, troop movement as a vertical and Execution as the 2nd vertical- once they have control of communication everything else follows- yjey demand control of the base, the pillar of support. Tid-Bits offered as “Permission to speak Sir” is the prime example of this sort of control. Distorting reality is a big part of the Military picture ( a Military graphic is used to set the soldier mind up for compliance- it is conveyed thryu words, pictures and exercise , enforced with disciplinary action). Our common Judiciary works the same way, e.g. : the Judge looks down at the plaintiff Veteran and says, Mr Jones, “it’s not your time to speak”, at that moment You are censored before you get a chance to speak ( supposedly in deference to rules of order, protocol and acquiescence to the court). We know this is abuse on the plaintiff- they consider us Plebes at the best.
I will say that once you put the soldier into a man , you cannot take it out and the soldier is no longer a Plebe ( commoner), and tough shit the VA if they don’t like that I expose their tactics ( I have a spread sheet of this stuff)
While I believe in the precepts of a civil society I also believe that soldiers should know why they are doing what they do and that all constitutional rights should be retained. Where our rights have been suspended for military purposes, if the soldier is harmed then a just debt is owed by the US Govt. ( the American People). We are not the sacrificial lambs of the Republic. I demand respect as a citizen and I return it because I believe in the Republic and why it was formed. When the chain of command believes it is losing control over the interface they apply an intervention like removing the cell phones. When a VA Psychiatrist deliberately under rates pathology to deny a claim, this is an example of using the semantic interface to beat down the Veteran, e.g. organic neurological disorder. When the VBA generates codified language and hires lawyers to double speak that language at the Veteran they are doing the same thing- disassembling reality to fit their own needs. The controllers at large will make up words and new names for invented disease categories as their nosology takes them to places they cannot defend.
Elf, I have read your words so many times and I am impressed with you as a person and as a Veteran who has struggled against he odds- I love you . Keep going at it because we need people like you to help steer the course. Eventually a leader will emerge from within the Veteran Community who will recognize a path toward restoring sanity because what we have now is just an outgrowth of the DOD mind control madness.
Yes agree with you Crazy Elf
The President according to Harry Truman
“The Buck stops Here”
No excuses!
I honestly believe that if you apply overwhelming numbers of Veterans who have all placed their signatures on a Document requesting such change, for all the reasons we all complain to one another about, we can get their attention, but it takes a “Never Stop Until We’re Dead” attitude. It takes not only pressure but continuos pressure on The White, Senators, Congressmen/women Democrats and Republicans) House and Senate VA Committee Chairmen, News, etc., until our Voice is heard and there is accountability and responsibility. We must be untied and not divided, and complete the mission at all cost.
The Cheyenne v.a. had such a screwed up mental health director that he was fired recently.
Nobody received any decent care under his tenure. He basically shut down the damned clinic. Hired complete idiots. And so forth.
I was told by a m.h. counselor that since there was no cure for my major depression and 3 distinct different types of severe P.T.S.D. then I could no longer be seen.
BULLSHIT!!!!! Goddammit!
The cheyenne v.a. is the absolute worst in the system due to its small size. Very small.
The whole hospital to include ALL of the clinics are rated at only a complexity level of 3 which is the lowest a hospital can go.
The employees mess with the patients constantly and have to be the absolute most stupid people on the planet. They definitely DO NOT know how to take care of people.
Being nice is definitely NOT in their playbook.
This just happened to me recently.
After giving blood at the small VA clinic. I asked if I was required to give a urine sample. Their answer was “…it hadn’t been ordered!”
I later called someone over this. The next Monday I gave the sample early. By 4:30 pm a “doctor” called and informed me of a “UTI”, (Urinary tract infection),! I asked about antibiotics.
Here’s the kicker;
This “alleged healthcare professional” stated: quote; “We don’t like giving out medications unless symptoms are present!” unquote!
My reply was, WHY? Because she had stated I did, in fact, have a UTI. Yet, even though I didn’t have the symptoms, shouldn’t she want to perform “preventive medicine”! Basically, “…preventing the UTI from becoming sepsis!”
That statement gave her the right to order me antibiotics!
If these comments are Valid than the
President should not be re-elected.
He has the money and the power and in his
first three years he could have fixed it.
He has done to correct the problem.
Big talk means BS.
@Daniel Cooney,
The VA is the second most corrupt government agency. Only surpassed by the DoD!
Top VA employees, SES’ers, have been caught stating, quote: “A President only serves 4 or 8 years. We can outlast them!”
Have you ever watched videos of the Veterans Committee in Washington. It’s a joke!
Lot’s of talk – only ABSOLUTELY NO ACTION!
For example: Your aware of how the dems have protected the identity of their whistleblower who’s against President Trump, right! Saying “…outing the name would put the person in jeopardy!”
That said, WHY aren’t they, or anyone, protecting the whistleblowers at the VA’s?
One, maybe more, have committed suicide because no one protected him from the upper managements!
I could go on. Only I hope you got the picture!
As we know, the Accountability Act is a joke and it does not give Veterans a voice or ability to file a legitimate complaint that should be then investigated and the wrong doer/s should be held responsible and accountable.
The only way this changes is stop complaining to each other and we need a website that will take our requests for change to the Chairmen of the Congress and Senate VA Committee/s. We can make change happen if we do it collectively and get mass numbers, and not through VA Service Organizations, and we also take it to the News. We need a leader to organize this so our complaints are finally heard loud and clear. I filed a FOIA request on any and all info letters, emails, notes, etc. the Houston VAMC Director had on me during a 1 year timeframe, and it came back with 151 Pages. I found out this VAMC Director, and suspect many more are doing the same, is utilizing VA Patient Advocates and Patient Relations employees to gather info on Veterans so the Director can respond to inquires. I have since sent this to the VA OIG, and there is an investigation as I understand it. How wrong does it get to use Patient Advocates, whose purpose is to help and protect Patient Rights, now to have them used against a Patient and/or Veteran.
Dr Edward H Hartnett Jr ,
Correction:
You stated, “The only way this changes is stop complaining to each other and we need a website that will take our requests for change to the Chairmen of the Congress and Senate VA Committee/s.”
It should read, “The only way this changes is stop complaining to each other and we need a website that will take our requests for change to the Chairmen of the House and Senate VA Committee/s.”
Congress has 2 chambers. One being the House of Representatives and the other being the Senate.
The president thinks they are the Congress and Senate too. Some other government officials too.
Can’t have a good government if they are stupid.
BTW, you have a good idea. It won’t work because the v.a. will shut it down somehow. A waste of time. Their screwed up union is THAT powerful! Shamefully.
I to am a patient at Minneapolis VA. I developed heart AFIB. I went to a local emergency room. I lived 80 miles from my GP in Ramsey, had to drive myself there. My GP called Minneapolis and he told me they wanted me to get there ASAP. I was retaining fluids to the point my shoes were stretched. They wanted to run tests and I would be spending the night. I showed up at the ER. I spent all of 2 minutes with a woman doctor who said give me a huge dose of diuretics and discharge me. When the nurse came with my paperwork she asked if I was OK. I told her no I was going home and kill myself. She said not to say that because if someone heard I would be put on hold. I left at 5:15 on a cold Friday night with 110 miles home. I was stuck in downtown traffic when I could not help myself and urinated all over me and my car. The had given me a urinal but there was no room for it. I drove all the way home constantly peeing and ruined my car seat. I was shivering and almost ran out of gas. I filed complaints twice and never got a response. I had to wait a few weeks to go back and get my heart under control, it was beating so fast but not moving blood. Thankfully a friend came and I did not take my life. After getting it under control with drugs I then had to wait months for a heart procedure. MY GP in Ramsey is good, and he cares but the VA as a whole is a mess. My mental health provider is also good. The delays in my heart procedure lead to lung problems. I could not keep up my yard anymore as I have also had 28 joint surgeries so I sold my house and took off in my RV to see the country. I was visiting a friend in North Carolina and could hardly breath so his wife took me to Fayetteville, NC emergency. The doctor gave me a treatment you breath in and an inhaler, the same one I had. HE NEVER EVEN LOOKED IN MY THROAT THOUGH I TOLD HIM IT WAS SWOLLEN. I left there sick and choking. I decided to come back to MN and saw my GP. He looked in my mouth and said I was full of Thrush. He gave me medication and told me it was actually a result of the Symbicort inhaler I was on. It says rinse your mouth after use. He told me that it’s a poor instruction, you need to brush your teeth and tounge. I just quit using it. I returned to my last trip of an old man and just returned to MN yesterday as I am buying another home. I am rated at 80% and my lawyers are trying to raise it. I haven’t been able to work since 2001. I have as I said had 28 joint surgeries, 10 spine alone with 4 discs fused. I had a staph infection after my hip 2nd replacement and destroyed so much muscle and I lived with no hip for 5 months. Before the VA I had doctors tell me I have abnormally soft cartiledge which caused this, but the VA takes each joint separately and doesn’t look at the system cause. I still have breathing troubles and have told them I worked in replacing old asbestos on ships and breathed in tons of dust, but they never even checked. I have reached the point where I am just enjoying the time I have left. The only time I ever feel desperate is dealing with the VA. It is my opinion that the VA has a suicide problem and they have caused it by how they treat us.
Steve,
The episode you described above with the care you received is blatant malpractice. The standard of care for what you described may have called for a diuretic but the abrupt discharge was improper. Lasix by IV causes rapid water loss, by pill it is slower but massive doses carry risks by either route: oral , IV or rectal. The risks include everything you describe but add to that, potential for electrolyte imbalance, hypotension, cardiac insufficiency , neurological problems (coma), how about precipitating a seizure, a heart attack ?
You should have been admitted and observed or given the dose to TAKE AT HOME where you can monitor your I/O’s ( inputs and outputs) , measure your weight loss, perform routine blood pressures and consume adequate amounts of fluids and electrolytes. A Nurse should have followed up with you.
I am glad you are at a point where you can enjoy what is left. Peace, Brother.
Well Ben we hope you offer this veterans family legal assistance because noone will be held accountable and they will blame the dead veteran
My husband was at the mishawaka Indiana Va the same day a veteran blew there head off. Va came out told veterans to ask for help get it authorized than denies all the Bill’s. My husband withdrew from va they have failed him and hold noone accountable. Criminal organization
Hey Ben,
I just read the “Independent Assessment of the Health Care Delivery Systems and Management Processes of the Department of Veterans Affairs” its a Snow-job on how to improve the VHA with emphasis on GOVERNANCE, MANAGEMENT, REORGANIZATION and TOOLS.
No Veteran input whatsoever but they keep pushing this crap like its the answer to fixing the VA Healthcare System. The TOOLS part is particularly interesting as it’s core is IT. Combine IT wit AI modules designed to promote better outcomes — but for Whom?
A lot of money is being spent on management and governance, I don;t see emphasis real Human Improvements in Patient Safety, Work Flow redesign, autonomy of practice or discipline. And of course the concept of Customer Service is and always has been missing.
In 2015 the Institute of Medicine renamed itself NAM ( National Academies of Medicine), all that stuff about crossing the “Quality Chasm” and To Err is Human” has vanished with hyperbole about Governance. The idea that privatization is going to happen appears muted. The redesign of the Veterans Health Administration Central Office (VHACO) just means more jobs for cronies and pay raises with year end bonuses coupled to reduction in care.
I’ll say it again, the VA is the face of Evil.
Anosognosia, an incurable organic neurological disease not listed in the DSM-5. Yes, the VA is lying and vets are dying.
Anosognosia is not in the DSM-5 because it is a neurological condition not a psychiatric condition, but has psychiatric manifestations like the tumor in the article above.
If the patient is unaware of having the neurological condition of anosognosia how is he supposed to adjust to having it. I discovered that anosognosia was a residual of my TBI in the winter of 1995. Of course I made no progress on my “adjustment disorder” until that discovery. After realizing that it was probably the root of my diagnosed adjustment disorder–organic personality disorder by then and after 3 hospitalizations for suicide ideation, I began to make headway on adjusting to the fact I couldn’t recognize the deficits in talents and skills that I had prior to my TBI. I felt like I was doing thing as well but someone or some thing was interfering with how the thing turned out.
Anosognosia also deprecates the reality check ability. What does it mean to your family if you take that finale exit? The question isn’t with the suicide ideation so the answer isn’t there either.
I repeat, anosognosia is incurable. I’ve had 2 hospitalizations for suicide ideation since 1995. I went to a PTSD (combined with my TBI) “CTP” group. Cognitive Therapy Program for PTSD designed to take vets off PTSD compensation for refusing to do the program. Of course, those of us in the group with anosognosia didn’t fit the program and were kicked out of the group by the third meeting. Out of 12, 3 were left.
I’ve never been compensated for PTSD. So it doesn’t apply to me in that way. It doesn’t do any good to write the VA or call the IG to try to lower the suicide rates by getting therapy properly directed. And so the lying and dying continue unabated. Not even Ben will take up the issue. No one wants to add another disability to the rating schedule for compensation.
Anosognosia, what are the symptoms and or indicators of this condition.
That’s the problem. The symptoms are not directly connected and are sometime vague. The individual themselves are often totally unaware of the problem but are blaming others and other things for their difficulties.
Thus the individual feels frustrated and depressed at things not turning out as well as his brain tells him they should.
The extreme is called unilateral neglect. A milder form is induced by alcohol. In the extreme, a woman was questioned by the Dr. in the article I read, “Whose hand is that on your lap?” It was the ladies left hand but she responded that it must be her sisters. Her sister must have left it on her visit yesterday. In the milder transient form caused by alcohol you’ve probably seen the surprise study participants have when watching video of driving through a cone path after having four ounces of alcohol. Previously they had driven the same route sober and the video showed no cones being run over.
My mother-in-law who had a right side stroke couldn’t remember she was paralyzed on the left side and would fall when she tried to stand up from her wheel chair.
If that doesn’t give you the picture, ask for more.
DSM-5 is the latest iteration by the American Psychological Association. As a not so simple man I can appreciate good work but DSM-5 is a nightmare. I looked at DSM-3 as an undergrad and thought is was comprehensive as a Tool goes. That version had roughly 64 pathologies. DSM-4 was never really rolled out.
DSM-5 has 350 different pathologies and everything is digitized with a spectrum for every manifestation of human behavior imaginable. This way its easy for Dr Ignuts to take your facial recognition scan and tie it to a cluster of clinical horse shit which will follow you everywhere you go- they have your face digitized . It is the computer they use in the exam room that is the front end of the DSM-5 Beast. Have you ever been to a VA Psychiatric appointment? With DSM-5 they have a disease category for everybody so if your not nuts they can figure out something for you. That Veterans go without care is inexcusable by this standard because DSM-5 has a nut job diagnosis for everyone, it just needs to be applied. Denial of care protocol is at the root of the VA Care model.
This reads like it has all the right words for a cold, calculating, ass-covering bureaucracy. They may just replace the word veteran with yardstick, given the compassion it lacks.
Hey, I did everything right and documented it 40 ways to Sunday, I did my job, but not any more than my job, but gee we are sorry that yardstick broke.
I had surgery at the new VA hospital in Denver last year. I was told to arrive early to check in the day prior. So I got there 3 hours early before that particular waiting area closed. I was met by a gentleman who worked there, and told to take a seat in the waiting room. I waited and watched dozens of patients go ahead of me.
My name was never called, I was left sitting in the room while they closed. About an hour after they closed, the last worker to leave saw me and asked me why I was still sitting there.
I told him I was never called, and hadn’t realized they had closed and locked up. I was physically locked up and forgotten.
There is no doubt in my mind it was intentional. The head of that department was called in, questioned me about what had happened and apologized profusely, she knew exactly who was responsible, and what had taken place.
Also, I was promised I would not have mesh implanted in my stomach by the surgeon, while laying groggy in the recovery room, the surgeon informed me he in fact, used it, against my will.
A few years ago, I was taken off opioid medication which I had been on for decades. Luckily I still had a primary physician who helped wean me off with patches.
Not long after that, health net, refused to pay for my care, which was authorized through the choice program.
I’m lucky now to once again receive my pain management, thru triwest and a pain specialist outside the VA. It was a 2 hour drive to receive inferior treatment at the VA hospital.
It’s still a major hassle to get treatments approved however, even though I’m 100% P&T service connected . Perhaps someday we will be given a medical card that will be accepted by any provider outside the VA.
“Medical cards” As long as all of the veteran organizations lobby against it, that will never happen.
How sad that the va system fails all of us Veterans! But the good Lord sees Everything! He says Do unto others as you want others to Do unto you!?
Benjamin, I had made the comment about not replying because my input means nothing. I am a gnat. However, though, I can say without being present at that location and without even knowing Brian Lewis, his comments are applicable to most VA facilities in regards to mental health. Here is why I say this. Because the evidence based practice dates back years and years. Ben even the VA formulary for cancer drugs has drugs on it that were used back in the 70s. The VA prescribes FDA Black Box Listed Medications that are banned in other countries. Yes Ben, follow up and you will see. I have mentioned this over and over; but, the people who can change policies, laws, and procedures view me as a gnat or non-existent. Remember, when you put an article out last spring about how different parts of the brain can regenerate themselves such as the memory located in the hippocampus. Ben, this information was put out in 2019 by the VA. This is old information. They have already been knowing this for 15+ years. This is what I mean. They keep pretending to evaluate and research like they are coming up with something new to tell the veterans or whomever. All spin Ben. No results. Here is another reason why I say the VA is losing in the mental health debate. This has to do with the VA secretaries shifting the mental health towards Telepsychiatry. If you desire to read about the truth regarding this type care, look up Volume 94, Number 12, December 2019 issue of the Mayo Clinic Proceedings. An article is written reviewing this type mental health care. “Barriers to the use of Telepsychiatry” is the name of the article. It is all about money. They do not give a shit. So why waste time and energy in death care? The people in charge believe they know it all. So why bother with them? Because all the rules, regulations, and laws are there to benefit themselves. Waste of money and time.
That disregard is probably rampant in all VA’s. I am not against anyone, though I must say, the influx of foreigners who refuse to acclimate to the culture of the people they are treating. That is definitely part of the issue. And the fact that American physicians will not get involved with the VA, well that is an issue too. But the foreigners in Austin TX VA go only by childlike textbook diagnosis’ and do not look any further than their tea leaves to prescribe, and if you do not see their specialist, then they will and do refuse vital medicine for your survival. That should not be allowed. They are more concerned with holding their position and power, than the oath for helping someone regain/stablize their health.
Austin TX VA has refused me two critical meds for my survival, which then does nothing for a trusting relationship between myself and them, yet, I must stay tethered to them. And then there is the VA claim, God bless what a mess.
We have tried to go to liaison, only to be mocked, changed doctors, and still get threatened by them if you do not see so and so, we will have to discontinue this med, then that one. Then in the same breath they are trying to sell you their wellness center, and outstanding psychiatric care they have to offer.
Thank God my hubby is able to afford my healthcare, VA, isn’t interested in providing it.
I have dealt with the VA at Austin, Cedar Park, Temple, and DBeeallas. The problems you have described I have experienced at all the places I listed. I have come to the conclusion that it is a problem caused or directed by VISN-17 so that they can report nothing but positive results against some measurement that they are reviewed on.
Been trying to come up with some way to expose the management of this VISN that can not be changed, erased, or lied about.
a recent article indicated 70% of all US Physicians have done some work for or with the VA at some time in the career. Many while in medical school.
IMO, many VA employees, who never served or never saw combat, have “distain for veterans”! They see us as someone receiving something for free! Which is contrary to those who have to pay for their healthcare.
Then we have the VA employees who are wanting to assist veterans in their healthcare. Yet, when they see a vet getting screwed – say nothing! IMO, these individuals ARE worse than the ones committing the malpractice! Because these individuals are “enabling these actions”!
What can be done about it, seems to be the main question! I suggest veterans be given a healthcare card. (Like a medicare card.) Where he/she can use it anywhere!
Or, like some have suggested. Use Champva for our healthcare! Basically it’s the same thing!
Lastly, those healthcare providers, in the VA healthcare system, who are found to be incompetent or otherwise – need to be fired and replaced immediately, not later on! If they are complicit in the death of a veteran, they should be held accountable!
I started going to the VA over 40 years after I came home from nam when the affordable healthcare become law and I lost my insurance and could not afford the replacement. Under VA care I had a heart attach my doctor did read the CT scan that I took to him .I have had galdbladder and two hernia and heart attach in three years under VA care all at my expence . All in all the VA elite are so full of hate ,anger and racest . I finally aged into Medicare and survived the VA.
This makes me so sad my husband is a Vietnam vet he has PTSD n all sorts of issue agent orange he had lung cancer n colon cancer this past year that to say this when my husband goes into all but 2 appt I go with him n I ask so many who what why n I dont think so. But I have to say we go to the small clinic in Newark Ohio n most stuff we go to Champler P Wyler in Columbus Ohio at both facilities have went above n beyond for him we have the best of the best of VA facilities. Then when. It comes to my husband I am his protector n he is mine it hasn’t been an easy road 49 years of night time screamed n days of withdraws but I pushed n ask what’s going on we had good days n bad but he is here n as of 5 yrs ago he stopped drinking s.oking n drugs n is now a Christian I never gave up praying. The Prayer of a reverent man reveals much never never give up
Thank you dear lady.
I never gave up on God and I’m still alive because of this. Tell your husband he’s loved by the Veteran Community.
Honestly, Benjamin, did the VA ever harass Former Senator John McCain? I respect his passing and it is not appropriate for me to bring this up. However, I have brought the issue up. I am bringing this up because there is a double standard in this country and it needs to stop.
Soon we might receive the Caregiver stipend post 9/11 receive. That will help
Paula, this is positive. I ? will remember your situation in my prayers. Best.
Benjamin, with the way that I have been shit on by the federal government, I do not give a damn if the current President, the DOJ, and the Supreme Court dismantles the whole federal government to remove the corruption. Then, start over fresh. This is my opinion.
Oh yes, I meant to add this. They cannot engage in alternative practices. They can only engage in what they are supposedly licensed under and what they have supposedly been educated under. Though, this is what they claim. We have to follow our laws. They say this but in many cases they do what they want too as long as they do not buck their leadership. Benjamin, I do not care what they do. It is going to take a Supreme Court iron fist decision to change this culture and an elimination of the AFGE union. If the AFGE union was eliminated, then the government employees would be on the same page as the non- government workers. They would have to pay for their own attorneys and purchase their own malpractice insurance. Thus, positive change might then start to profilerate throughout the veteran consumer community.
My last point-the VA decide-not hardly. When I had been involved in straightening up and cleaning up behind them in the recent years, please give me a damn break. The VA can go straight to hell. God may not like my choice of words. Though he might with how his children of God have been and are being treated. ?
In my opinion, Republican Tom Cotton should run for the presidency in 2024. He is a low keyed upright Republican.
He stands tall no matter what. ??? Research and view why I say this.